


What the Next 18 Months Can Look Like, if Leaders Buy Us Time


Coronavirus from SARS isolated in FRhK-4 cells. Thin section electron micrograph and negative stained virus particles
If you are an expert in the field and want to criticize or endorse the article or some of its parts, feel free to leave a private note here or contextually and I will respond or address.
If you want to translate this article, do it on a Medium post and leave me a private note here with your link. Here are the translations currently available:
Spanish (verified by author, full translation inc. charts)(alt. vs. 1, 2, 3, 4, 5, 6)French (translated by an epidemiologist)
Chinese Traditional (full translation including charts, alternative translation)Chinese Simplified
German
Portuguese (alternative version)Russian
Italian (with graphs translated)(Alternative 1, Alternative version on Facebook)
Japanese
Vietnamese
Turkish
Polish
Icelandic (alternative translation)Greek
Bahasa Indonesia
Bahasa Malaysia
Farsi (alternative version outside of Medium)
Czech (alternative translation)Dutch
Norwegian
Hebrew
Ukrainian (alternative version)Swedish
Romanian (alternative version)Bulgarian
Catalonian
Slovak
Filipino
Hungarian (Alternative, with part 1, part 2)
Chinese Traditional (full translation including charts, alternative translation)Chinese Simplified
German
Portuguese (alternative version)Russian
Italian (with graphs translated)(Alternative 1, Alternative version on Facebook)
Japanese
Vietnamese
Turkish
Polish
Icelandic (alternative translation)Greek
Bahasa Indonesia
Bahasa Malaysia
Farsi (alternative version outside of Medium)
Czech (alternative translation)Dutch
Norwegian
Hebrew
Ukrainian (alternative version)Swedish
Romanian (alternative version)Bulgarian
Catalonian
Slovak
Filipino
Hungarian (Alternative, with part 1, part 2)
Mar 19 · 29 min read
This article follows Coronavirus: Why You Must Act Now, with over 40 million views and 30 translations. If you agree with this article, consider signing the corresponding White House petition. Translations available in 29 languages at the bottom. Running list of endorsements here. 9 million views so far.
Summary of the article: Strong coronavirus measures today should only last a few weeks, there shouldn’t be a big peak of infections afterwards, and it can all be done for a reasonable cost to society, saving millions of lives along the way. If we don’t take these measures, tens of millions will be infected, many will die, along with anybody else that requires intensive care, because the healthcare system will have collapsed.
Within a week, countries around the world have gone from: “This coronavirus thing is not a big deal” to declaring the state of emergency. Yet many countries are still not doing much. Why?
Every country is asking the same question: How should we respond? The answer is not obvious to them.
Some countries, like France, Spain or Philippines, have since ordered heavy lockdowns. Others, like the US, UK, or Switzerland, have dragged their feet, hesitantly venturing into social distancing measures.
Here’s what we’re going to cover today, again with lots of charts, data and models with plenty of sources:
- What’s the current situation?
- What options do we have?
- What’s the one thing that matters now: Time
- What does a good coronavirus strategy look like?
- How should we think about the economic and social impacts?
When you’re done reading the article, this is what you’ll take away:
Our healthcare system is already collapsing.
Countries have two options: either they fight it hard now, or they will suffer a massive epidemic.
If they choose the epidemic, hundreds of thousands will die. In some countries, millions.
And that might not even eliminate further waves of infections.
If we fight hard now, we will curb the deaths.
We will relieve our healthcare system.
We will prepare better.
We will learn.
The world has never learned as fast about anything, ever.
And we need it, because we know so little about this virus.
All of this will achieve something critical: Buy Us Time.
Countries have two options: either they fight it hard now, or they will suffer a massive epidemic.
If they choose the epidemic, hundreds of thousands will die. In some countries, millions.
And that might not even eliminate further waves of infections.
If we fight hard now, we will curb the deaths.
We will relieve our healthcare system.
We will prepare better.
We will learn.
The world has never learned as fast about anything, ever.
And we need it, because we know so little about this virus.
All of this will achieve something critical: Buy Us Time.
If we choose to fight hard, the fight will be sudden, then gradual.
We will be locked in for weeks, not months.
Then, we will get more and more freedoms back.
It might not be back to normal immediately.
But it will be close, and eventually back to normal.
And we can do all that while considering the rest of the economy too.
We will be locked in for weeks, not months.
Then, we will get more and more freedoms back.
It might not be back to normal immediately.
But it will be close, and eventually back to normal.
And we can do all that while considering the rest of the economy too.
Ok, let’s do this.
1. What’s the situation?
Last week, I showed this curve:
It showed coronavirus cases across the world outside of China. We could only discern Italy, Iran and South Korea. So I had to zoom in on the bottom right corner to see the emerging countries. My entire point is that they would soon be joining these 3 cases.
Let’s see what has happened since.

As predicted, the number of cases has exploded in dozens of countries. Here, I was forced to show only countries with over 1,000 cases. A few things to note:
- Spain, Germany, France and the US all have more cases than Italy when it ordered the lockdown
- An additional 16 countries have more cases today than Hubei when it went under lockdown: Japan, Malaysia, Canada, Portugal, Australia, Czechia, Brazil and Qatar have more than Hubei but below 1,000 cases. Switzerland, Sweden, Norway, Austria, Belgium, Netherlands and Denmark all have above 1,000 cases.
Do you notice something weird about this list of countries? Outside of China and Iran, which have suffered massive, undeniable outbreaks, and Brazil and Malaysia, every single country in this list is among the wealthiest in the world.
Do you think this virus targets rich countries? Or is it more likely that rich countries are better able to identify the virus?
It’s unlikely that poorer countries aren’t touched. Warm and humid weather probably helps, but doesn’t prevent an outbreak by itself — otherwise Singapore, Malaysia or Brazil wouldn’t be suffering outbreaks.
The most likely interpretations are that the coronavirus either took longer to reach these countries because they’re less connected, or it’s already there but these countries haven’t been able to invest enough on testing to know.
Either way, if this is true, it means that most countries won’t escape the coronavirus. It’s a matter of time before they see outbreaks and need to take measures.
What measures can different countries take?
2. What Are Our Options?
Since the article last week, the conversation has changed and many countries have taken measures. Here are some of the most illustrative examples:
Measures in Spain and France
In one extreme, we have Spain and France. This is the timeline of measures for Spain:
On Thursday, 3/12, the President dismissed suggestions that the Spanish authorities had been underestimating the health threat.
On Friday, they declared the State of Emergency.
On Saturday, measures were taken:
On Friday, they declared the State of Emergency.
On Saturday, measures were taken:
- People can’t leave home except for key reasons: groceries, work, pharmacy, hospital, bank or insurance company (extreme justification)
- Specific ban on taking kids out for a walk or seeing friends or family (except to take care of people who need help, but with hygiene and physical distance measures)
- All bars and restaurants closed. Only take-home acceptable.
- All entertainment closed: sports, movies, museums, municipal celebrations…
- Weddings can’t have guests. Funerals can’t have more than a handful of people.
- Mass transit remains open
On Monday, land borders were shut.
Some people see this as a great list of measures. Others put their hands up in the air and cry of despair. This difference is what this article will try to reconcile.
France’s timeline of measures is similar, except they took more time to apply them, and they are more aggressive now. For example, rent, taxes and utilities are suspended for small businesses.
Measures in the US and UK
The US and UK, like countries such as Switzerland, have dragged their feet in implementing measures. Here’s the timeline for the US:
- Wednesday 3/11: travel ban.
- Friday: National Emergency declared. No social distancing measures
- Monday: the government urges the public to avoid restaurants or bars and attend events with more than 10 people. No social distancing measure is actually enforceable. It’s just a suggestion.
Lots of states and cities are taking the initiative and mandating much stricter measures.
The UK has seen a similar set of measures: lots of recommendations, but very few mandates.
These two groups of countries illustrate the two extreme approaches to fight the coronavirus: mitigation and suppression. Let’s understand what they mean.
Option 1: Do Nothing
Before we do that, let’s see what doing nothing would entail for a country like the US:
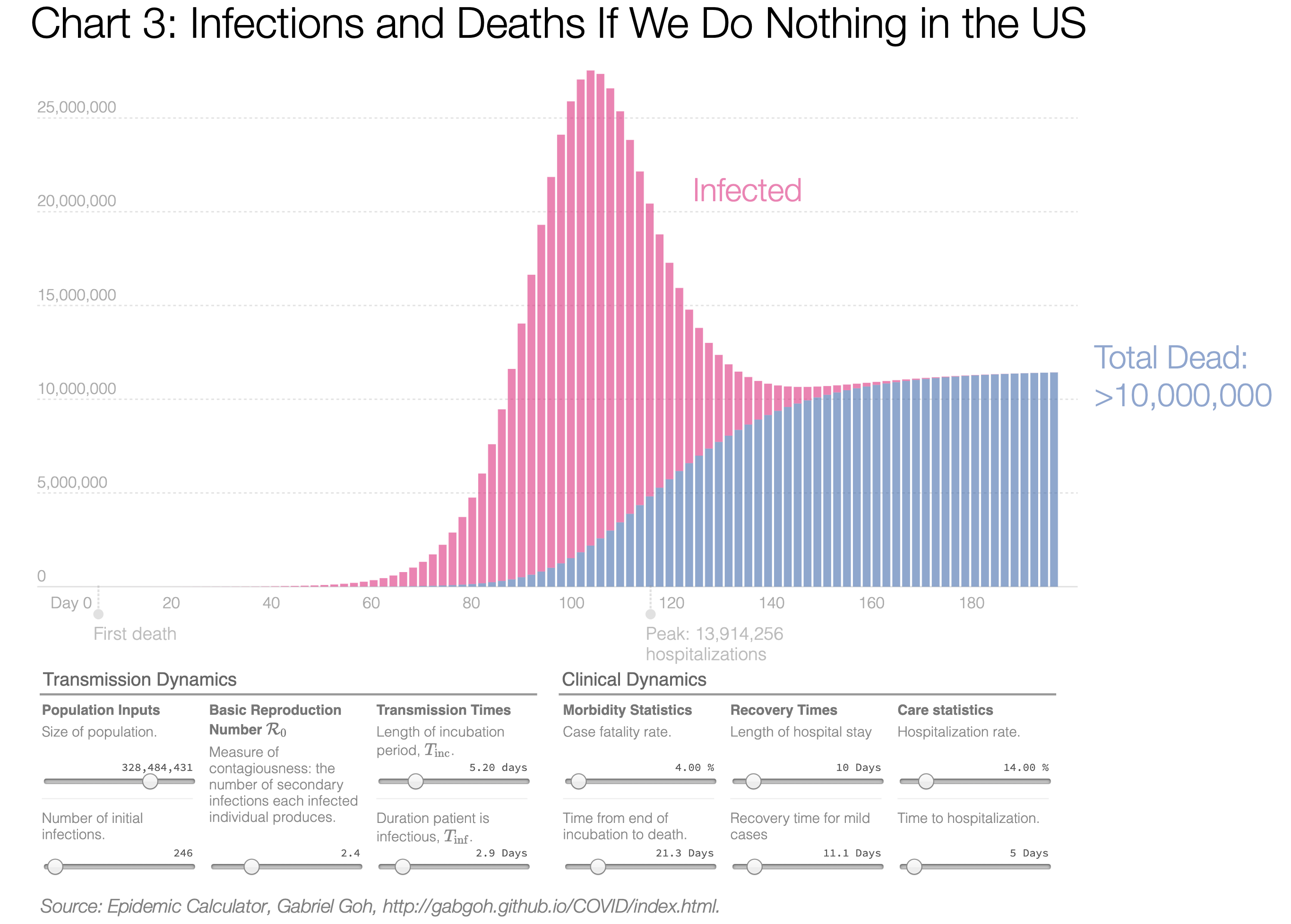
This fantastic epidemic calculator can help you understand what will happen under different scenarios. I’ve pasted below the graph the key factors that determine the behavior of the virus. Note that infected, in pink, peak in the tens of millions at a certain date. Most variables have been kept from the default. The only material changes are R from 2.2 to 2.4 (corresponds better to currently available information. See at the bottom of the epidemic calculator), fatality rate (4% due to healthcare system collapse. See details below or in the previous article), length of hospital stay (down from 20 to 10 days) and hospitalization rate (down from 20% to 14% based on severe and critical cases. Note the WHO calls out a 20% rate) based on our most recently available gathering of research. Note that these numbers don’t change results much. The only change that matters is the fatality rate.
If we do nothing: Everybody gets infected, the healthcare system gets overwhelmed, the mortality explodes, and ~10 million people die (blue bars). For the back-of-the-envelope numbers: if ~75% of Americans get infected and 4% die, that’s 10 million deaths, or around 25 times the number of US deaths in World War II.
You might wonder: “That sounds like a lot. I’ve heard much less than that!”
So what’s the catch? With all these numbers, it’s easy to get confused. But there’s only two numbers that matter: What share of people will catch the virus and fall sick, and what share of them will die. If only 25% are sick (because the others have the virus but don’t have symptoms so aren’t counted as cases), and the fatality rate is 0.6% instead of 4%, you end up with 500k deaths in the US.
If we don’t do anything, the number of deaths from the coronavirus will probably land between these two numbers. The chasm between these extremes is mostly driven by the fatality rate, so understanding it better is crucial. What really causes the coronavirus deaths?
How Should We Think about the Fatality Rate?
This is the same graph as before, but now looking at hospitalized people instead of infected and dead:
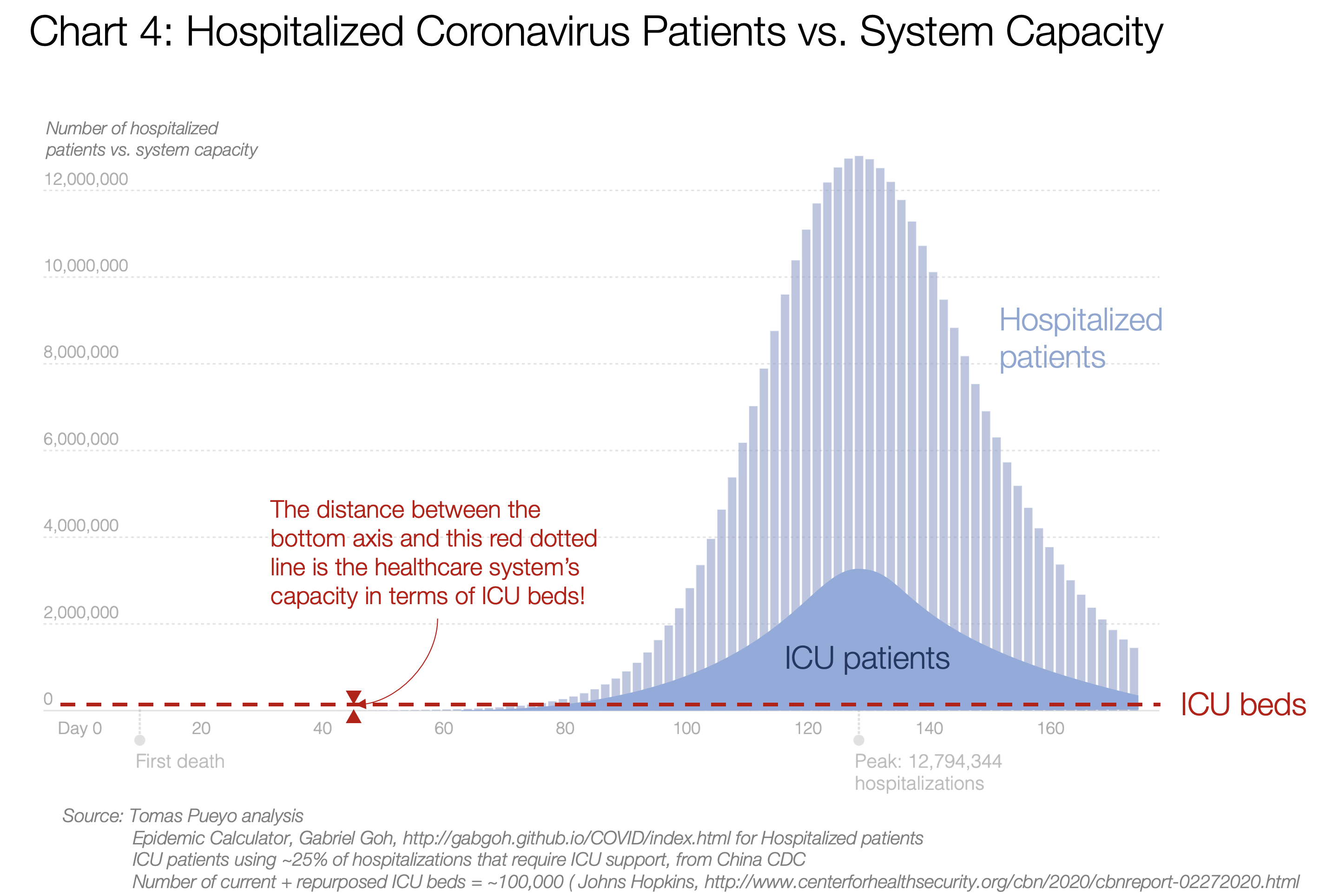
The light blue area is the number of people who would need to go to the hospital, and the darker blue represents those who need to go to the intensive care unit (ICU). You can see that number would peak at above 3 million.
Now compare that to the number of ICU beds we have in the US (50k today, we could double that repurposing other space). That’s the red dotted line.
No, that’s not an error.
That red dotted line is the capacity we have of ICU beds. Everyone above that line would be in critical condition but wouldn’t be able to access the care they need, and would likely die.
Instead of ICU beds you can also look at ventilators, but the result is broadly the same, since there are fewer than 100k ventilators in the US.
This is why people died in droves in Hubei and are now dying in droves in Italy and Iran. The Hubei fatality rate ended up better than it could have been because they built 2 hospitals nearly overnight. Italy and Iran can’t do the same; few, if any, other countries can. We’ll see what ends up happening there.
So why is the fatality rate close to 4%?
If 5% of your cases require intensive care and you can’t provide it, most of those people die. As simple as that.
Additionally, recent data suggests that US cases are more severe than in China.
I wish that was all, but it isn’t.
Collateral Damage
These numbers only show people dying from coronavirus. But what happens if all your healthcare system is collapsed by coronavirus patients? Others also die from other ailments.
What happens if you have a heart attack but the ambulance takes 50 minutes to come instead of 8 (too many coronavirus cases) and once you arrive, there’s no ICU and no doctor available? You die.
There are 4 million admissions to the ICU in the US every year, and 500k (~13%) of them die. Without ICU beds, that share would likely go much closer to 80%. Even if only 50% died, in a year-long epidemic you go from 500k deaths a year to 2M, so you’re adding 1.5M deaths, just with collateral damage.
If the coronavirus is left to spread, the US healthcare system will collapse, and the deaths will be in the millions, maybe more than 10 million.
The same thinking is true for most countries. The number of ICU beds and ventilators and healthcare workers are usually similar to the US or lower in most countries. Unbridled coronavirus means healthcare system collapse, and that means mass death.
Unbridled coronavirus means healthcare systems collapse, and that means mass death.
By now, I hope it’s pretty clear we should act. The two options that we have are mitigation and suppression. Both of them propose to “flatten the curve”, but they go about it very differently.
Option 2: Mitigation Strategy
Mitigation goes like this: “It’s impossible to prevent the coronavirus now, so let’s just have it run its course, while trying to reduce the peak of infections. Let’s just flatten the curve a little bit to make it more manageable for the healthcare system.”
This chart appears in a very important paper published over the weekend from the Imperial College London. Apparently, it pushed the UK and US governments to change course.
It’s a very similar graph as the previous one. Not the same, but conceptually equivalent. Here, the “Do Nothing” situation is the black curve. Each one of the other curves are what would happen if we implemented tougher and tougher social distancing measures. The blue one shows the toughest social distancing measures: isolating infected people, quarantining people who might be infected, and secluding old people. This blue line is broadly the current UK coronavirus strategy, although for now they’re just suggesting it, not mandating it.
Here, again, the red line is the capacity for ICUs, this time in the UK. Again, that line is very close to the bottom. All that area of the curve on top of that red line represents coronavirus patients who would mostly die because of the lack of ICU resources.
Not only that, but by flattening the curve, the ICUs will collapse for months, increasing collateral damage.
You should be shocked. When you hear: “We’re going to do some mitigation” what they’re really saying is: “We will knowingly overwhelm the healthcare system, driving the fatality rate up by a factor of 10x at least.”
You would imagine this is bad enough. But we’re not done yet. Because one of the key assumptions of this strategy is what’s called “Herd Immunity”.
Herd Immunity and Virus Mutation
The idea is that all the people who are infected and then recover are now immune to the virus. This is at the core of this strategy: “Look, I know it’s going to be hard for some time, but once we’re done and a few million people die, the rest of us will be immune to it, so this virus will stop spreading and we’ll say goodbye to the coronavirus. Better do it at once and be done with it, because our alternative is to do social distancing for up to a year and risk having this peak happen later anyways.”
Except this assumes one thing: the virus doesn’t change too much. If it doesn’t change much, then lots of people do get immunity, and at some point the epidemic dies down
How likely is this virus to mutate?
It seems it already has.
It seems it already has.
This graph represents the different mutations of the virus. You can see that the initial strains started in purple in China and then spread. Each time you see a branching on the left graph, that is a mutation leading to a slightly different variant of the virus.
This should not be surprising: RNA-based viruses like the coronavirus or the flu tend to mutate around 100 times faster than DNA-based ones—although the coronavirus mutates more slowly than influenza viruses.
Not only that, but the best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide: hundreds of millions of people infected.
That’s why you have to get a flu shot every year. Because there are so many flu strains, with new ones always evolving, the flu shot can never protect against all strains.
Put in another way: the mitigation strategy not only assumes millions of deaths for a country like the US or the UK. It also gambles on the fact that the virus won’t mutate too much — which we know it does. And it will give it the opportunity to mutate. So once we’re done with a few million deaths, we could be ready for a few million more — every year. This corona virus could become a recurring fact of life, like the flu, but many times deadlier.
The best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide.
So if neither doing nothing and mitigation will work, what’s the alternative? It’s called suppression.
Option 3: Suppression Strategy
The Mitigation Strategy doesn’t try to contain the epidemic, just flatten the curve a bit. Meanwhile, the Suppression Strategy tries to apply heavy measures to quickly get the epidemic under control. Specifically:
- Go hard right now. Order heavy social distancing. Get this thing under control.
- Then, release the measures, so that people can gradually get back their freedoms and something approaching normal social and economic life can resume.
What does that look like?
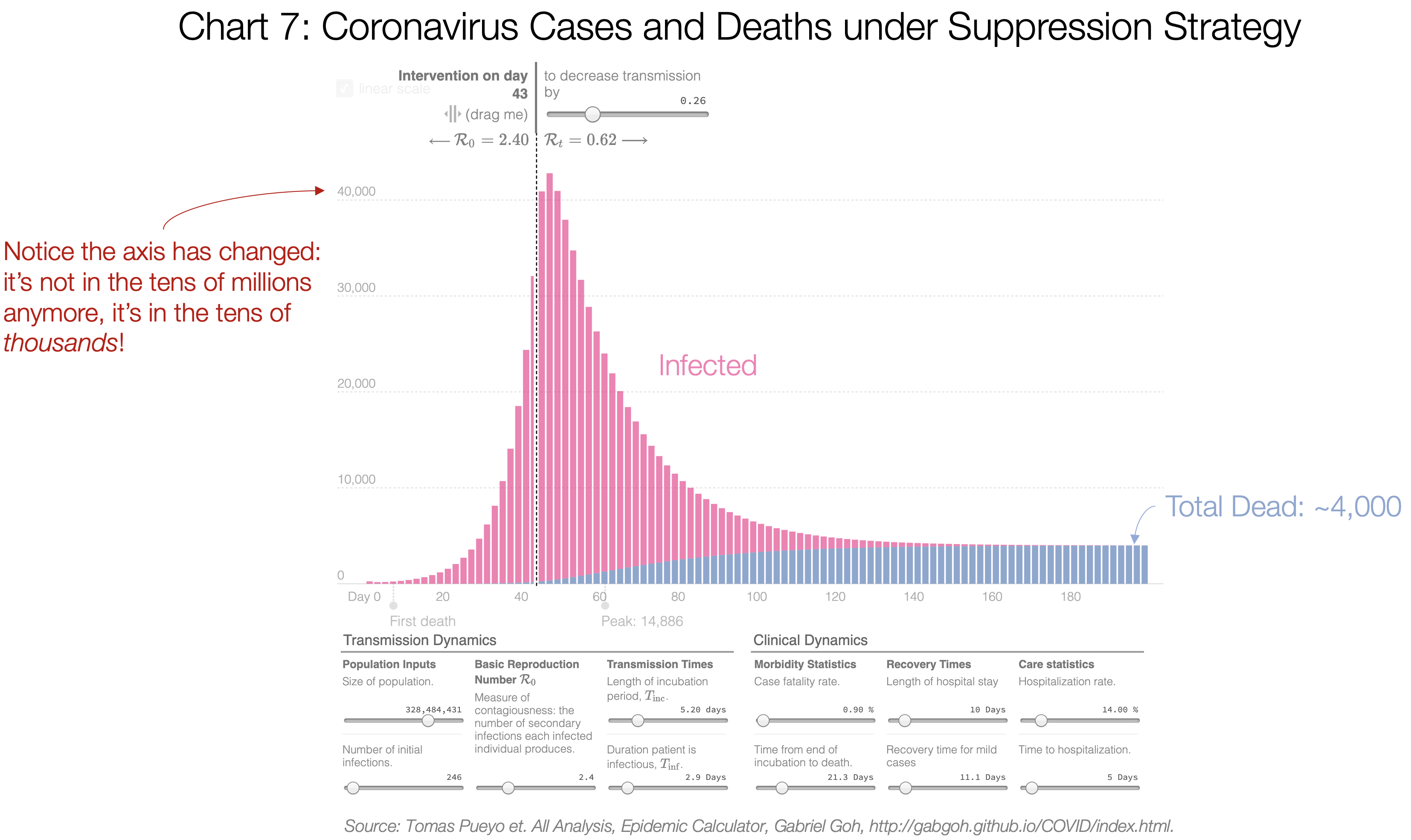
All the model parameters are the same, except that there is an intervention around now to reduce the transmission rate to R=0.62, and because the healthcare system isn’t collapsed, the fatality rate goes down to 0.6%. I defined “around now” as having ~32,000 cases when implementing the measures (3x the official number as of today, 3/19). Note that this is not too sensitive to the R chosen. An R of 0.98 for example shows 15,000 deaths. Five times more than with an R of 0.62, but still tens of thousands of deaths and not millions. It’s also not too sensitive to the fatality rate: if it’s 0.7% instead of 0.6%, the death toll goes from 15,000 to 17,000. It’s the combination of a higher R, a higher fatality rate, and a delay in taking measures that explodes the number of fatalities. That’s why we need to take measures to reduce R today. For clarification, the famous R0 is R at the beginning (R at time 0). It’s the transmission rate when nobody is immune yet and there are no measures against it taken. R is the overall transmission rate.
Under a suppression strategy, after the first wave is done, the death toll is in the thousands, and not in the millions.
Why? Because not only do we cut the exponential growth of cases. We also cut the fatality rate since the healthcare system is not completely overwhelmed. Here, I used a fatality rate of 0.9%, around what we’re seeing in South Korea today, which has been most effective at following Suppression Strategy.
Said like this, it sounds like a no-brainer. Everybody should follow the Suppression Strategy.
So why do some governments hesitate?
They fear three things:
- This first lockdown will last for months, which seems unacceptable for many people.
- A months-long lockdown would destroy the economy.
- It wouldn’t even solve the problem, because we would be just postponing the epidemic: later on, once we release the social distancing measures, people will still get infected in the millions and die.
Here is how the Imperial College team modeled suppressions. The green and yellow lines are different scenarios of Suppression. You can see that doesn’t look good: We still get huge peaks, so why bother?
We’ll get to these questions in a moment, but there’s something more important before.
This is completely missing the point.
Presented like these, the two options of Mitigation and Suppression, side by side, don’t look very appealing. Either a lot of people die soon and we don’t hurt the economy today, or we hurt the economy today, just to postpone the deaths.
This ignores the value of time.
3. The Value of Time
In our previous post, we explained the value of time in saving lives. Every day, every hour we waited to take measures, this exponential threat continued spreading. We saw how a single day could reduce the total cases by 40% and the death toll by even more.
But time is even more valuable than that.
We’re about to face the biggest wave of pressure on the healthcare system ever seen in history. We are completely unprepared, facing an enemy we don’t know. That is not a good position for war.
What if you were about to face your worst enemy, of which you knew very little, and you had two options: Either you run towards it, or you escape to buy yourself a bit of time to prepare. Which one would you choose?
This is what we need to do today. The world has awakened. Every single day we delay the coronavirus, we can get better prepared. The next sections detail what that time would buy us:
Lower the Number of Cases
With effective suppression, the number of true cases would plummet overnight, as we saw in Hubei last week.
Source: Tomas Pueyo analysis over chart and data from the Journal of the American Medical Association
As of today, there are 0 daily new cases of coronavirus in the entire 60 million-big region of Hubei.
The diagnostics would keep going up for a couple of weeks, but then they would start going down. With fewer cases, the fatality rate starts dropping too. And the collateral damage is also reduced: fewer people would die from non-coronavirus-related causes because the healthcare system is simply overwhelmed.
Suppression would get us:
- Fewer total cases of Coronavirus
- Immediate relief for the healthcare system and the humans who run it
- Reduction in fatality rate
- Reduction in collateral damage
- Ability for infected, isolated and quarantined healthcare workers to get better and back to work. In Italy, healthcare workers represent 8% of all contagions.
Understand the True Problem: Testing and Tracing
Right now, the UK and the US have no idea about their true cases. We don’t know how many there are. We just know the official number is not right, and the true one is in the tens of thousands of cases. This has happened because we’re not testing, and we’re not tracing.
- With a few more weeks, we could get our testing situation in order, and start testing everybody. With that information, we would finally know the true extent of the problem, where we need to be more aggressive, and what communities are safe to be released from a lockdown.
- New testing methods could speed up testing and drive costs down substantially.
- We could also set up a tracing operation like the ones they have in China or other East Asia countries, where they can identify all the people that every sick person met, and can put them in quarantine. This would give us a ton of intelligence to release later on our social distancing measures: if we know where the virus is, we can target these places only. This is not rocket science: it’s the basics of how East Asia Countries have been able to control this outbreak without the kind of draconian social distancing that is increasingly essential in other countries.
The measures from this section (testing and tracing) single-handedly curbed the growth of the coronavirus in South Korea and got the epidemic under control, without a strong imposition of social distancing measures.
Build Up Capacity
The US (and presumably the UK) are about to go to war without armor.
We have masks for just two weeks, few personal protective equipments (“PPE”), not enough ventilators, not enough ICU beds, not enough ECMOs (blood oxygenation machines)… This is why the fatality rate would be so high in a mitigation strategy.
But if we buy ourselves some time, we can turn this around:
- We have more time to buy equipment we will need for a future wave
- We can quickly build up our production of masks, PPEs, ventilators, ECMOs, and any other critical device to reduce fatality rate.
Put in another way: we don’t need years to get our armor, we need weeks. Let’s do everything we can to get our production humming now. Countries are mobilized. People are being inventive, such as using 3D printing for ventilator parts. We can do it. We just need more time. Would you wait a few weeks to get yourself some armor before facing a mortal enemy?
This is not the only capacity we need. We will need health workers as soon as possible. Where will we get them? We need to train people to assist nurses, and we need to get medical workers out of retirement. Many countries have already started, but this takes time. We can do this in a few weeks, but not if everything collapses.
Lower Public Contagiousness
The public is scared. The coronavirus is new. There’s so much we don’t know how to do yet! People haven’t learned to stop hand-shaking. They still hug. They don’t open doors with their elbow. They don’t wash their hands after touching a door knob. They don’t disinfect tables before sitting.
Once we have enough masks, we can use them outside of the healthcare system too. Right now, it’s better to keep them for healthcare workers. But if they weren’t scarce, people should wear them in their daily lives, making it less likely that they infect other people when sick, and with proper training also reducing the likelihood that the wearers get infected. (In the meantime, wearing something is better than nothing.)
All of these are pretty cheap ways to reduce the transmission rate. The less this virus propagates, the fewer measures we’ll need in the future to contain it. But we need time to educate people on all these measures and equip them.
Understand the Virus
We know very very little about the virus. But every week, hundreds of new papers are coming.
The world is finally united against a common enemy. Researchers around the globe are mobilizing to understand this virus better.
How does the virus spread?
How can contagion be slowed down?
What is the share of asymptomatic carriers?
Are they contagious? How much?
What are good treatments?
How long does it survive?
On what surfaces?
How do different social distancing measures impact the transmission rate?
What’s their cost?
What are tracing best practices?
How reliable are our tests?
How can contagion be slowed down?
What is the share of asymptomatic carriers?
Are they contagious? How much?
What are good treatments?
How long does it survive?
On what surfaces?
How do different social distancing measures impact the transmission rate?
What’s their cost?
What are tracing best practices?
How reliable are our tests?
Clear answers to these questions will help make our response as targeted as possible while minimizing collateral economic and social damage. And they will come in weeks, not years.
Find Treatments
Not only that, but what if we found a treatment in the next few weeks? Any day we buy gets us closer to that. Right now, there are already several candidates, such as Favipiravir, Chloroquine, or Chloroquine combined with Azithromycin. What if it turned out that in two months we discovered a treatment for the coronavirus? How stupid would we look if we already had millions of deaths following a mitigation strategy?
Understand the Cost-Benefits
All of the factors above can help us save millions of lives. That should be enough. Unfortunately, politicians can’t only think about the lives of the infected. They must think about all the population, and heavy social distancing measures have an impact on others.
Right now we have no idea how different social distancing measures reduce transmission. We also have no clue what their economic and social costs are.
Isn’t it a bit difficult to decide what measures we need for the long term if we don’t know their cost or benefit?
A few weeks would give us enough time to start studying them, understand them, prioritize them, and decide which ones to follow.
Fewer cases, more understanding of the problem, building up assets, understanding the virus, understanding the cost-benefit of different measures, educating the public… These are some core tools to fight the virus, and we just need a few weeks to develop many of them. Wouldn’t it be dumb to commit to a strategy that throws us instead, unprepared, into the jaws of our enemy?
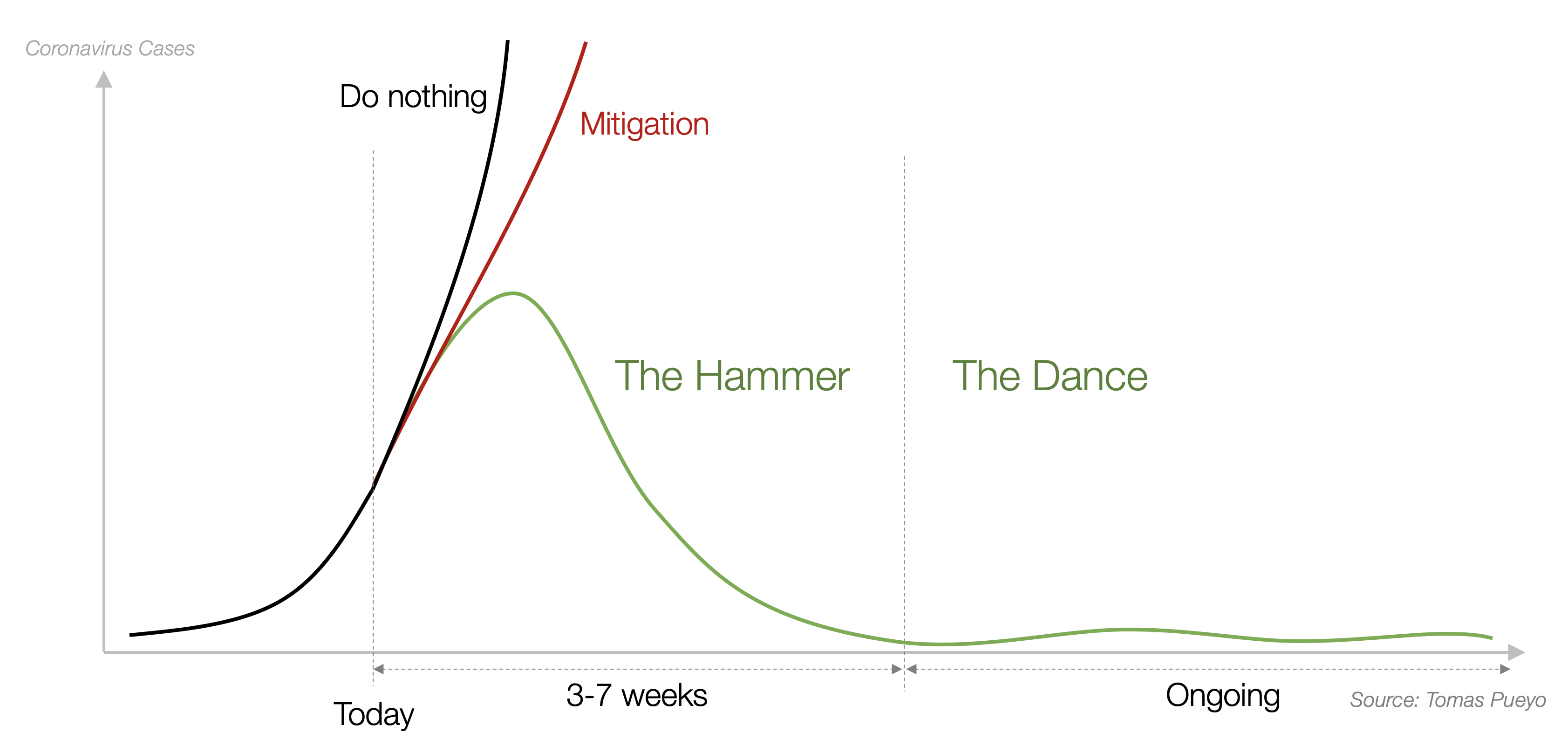
4. The Hammer and the Dance
Now we know that the Mitigation Strategy is probably a terrible choice, and that the Suppression Strategy has a massive short-term advantage.
But people have rightful concerns about this strategy:
- How long will it actually last?
- How expensive will it be?
- Will there be a second peak as big as if we didn’t do anything?
Here, we’re going to look at what a true Suppression Strategy would look like. We can call it the Hammer and the Dance.
The Hammer
First, you act quickly and aggressively. For all the reasons we mentioned above, given the value of time, we want to quench this thing as soon as possible.
One of the most important questions is: How long will this last?
The fear that everybody has is that we will be locked inside our homes for months at a time, with the ensuing economic disaster and mental breakdowns. This idea was unfortunately entertained in the famous Imperial College paper:
Do you remember this chart? The light blue area that goes from end of March to end of August is the period that the paper recommends as the Hammer, the initial suppression that includes heavy social distancing.
If you’re a politician and you see that one option is to let hundreds of thousands or millions of people die with a mitigation strategy and the other is to stop the economy for five months before going through the same peak of cases and deaths, these don’t sound like compelling options.
But this doesn’t need to be so. This paper, driving policy today, has been brutally criticized for core flaws: They ignore contact tracing (at the core of policies in South Korea, China or Singapore among others) or travel restrictions (critical in China), ignore the impact of big crowds…
The time needed for the Hammer is weeks, not months.
This graph shows the new cases in the entire Hubei region (60 million people) every day since 1/23. Within 2 weeks, the country was starting to get back to work. Within ~5 weeks it was completely under control. And within 7 weeks the new diagnostics was just a trickle. Let’s remember this was the worst region in China.
Remember again that these are the orange bars. The grey bars, the true cases, had plummeted much earlier (see Chart 9).
The measures they took were pretty similar to the ones taken in Italy, Spain or France: isolations, quarantines, people had to stay at home unless there was an emergency or had to buy food, contact tracing, testing, more hospital beds, travel bans…
Details matter, however.
China’s measures were stronger. For example, people were limited to one person per household allowed to leave home every three days to buy food. Also, their enforcement was severe. It is likely that this severity stopped the epidemic faster.
In Italy, France and Spain, measures were not as drastic, and their implementation is not as tough. People still walk on the streets, many without masks. This is likely to result in a slower Hammer: more time to fully control the epidemic.
Some people interpret this as “Democracies will never be able to replicate this reduction in cases”. That’s wrong.

For several weeks, South Korea had the worst epidemic outside of China. Now, it’s largely under control. And they did it without asking people to stay home. They achieved it mostly with very aggressive testing, contact tracing, and enforced quarantines and isolations.
The following table gives a good sense of what measures different countries have followed, and how that has impacted them (this is a work-in-progress. Feedback welcome.)

This shows how countries who were prepared, with stronger epidemiological authority, education on hygiene and social distancing, and early detection and isolation, didn’t have to pay with heavier measures afterwards.
Conversely, countries like Italy, Spain or France weren’t doing these well, and had to then apply the Hammer with the hard measures at the bottom to catch up.
The lack of measures in the US and UK is in stark contrast, especially in the US. These countries are still not doing what allowed Singapore, South Korea or Taiwan to control the virus, despite their outbreaks growing exponentially. But it’s a matter of time. Either they have a massive epidemic, or they realize late their mistake, and have to overcompensate with a heavier Hammer. There is no escape from this.
But it’s doable. If an outbreak like South Korea’s can be controlled in weeks and without mandated social distancing, Western countries, which are already applying a heavy Hammer with strict social distancing measures, can definitely control the outbreak within weeks. It’s a matter of discipline, execution, and how much the population abides by the rules.
Once the Hammer is in place and the outbreak is controlled, the second phase begins: the Dance.
The Dance
If you hammer the coronavirus, within a few weeks you’ve controlled it and you’re in much better shape to address it. Now comes the longer-term effort to keep this virus contained until there’s a vaccine.
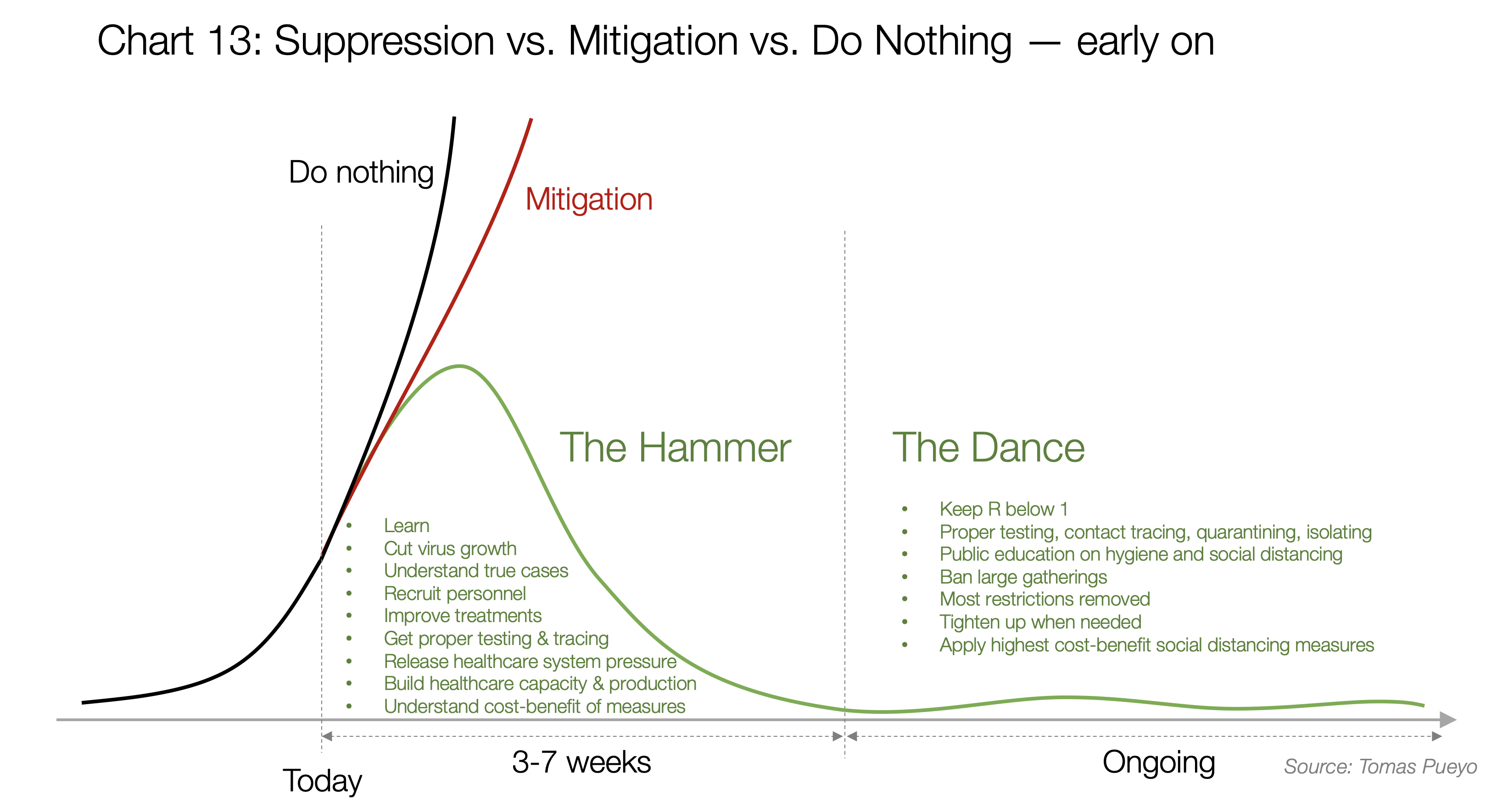
This is probably the single biggest, most important mistake people make when thinking about this stage: they think it will keep them home for months. This is not the case at all. In fact, it is likely that our lives will go back to close to normal.
The Dance in Successful Countries
How come South Korea, Singapore, Taiwan and Japan have had cases for a long time, in the case of South Korea thousands of them, and yet they’re not locked down home?
In this video, the South Korea Foreign Minister explains how her country did it. It was pretty simple: efficient testing, efficient tracing, travel bans, efficient isolating and efficient quarantining.
This paper explains Singapore’s approach:
Want to guess their measures? The same ones as in South Korea. In their case, they complemented with economic help to those in quarantine and travel bans and delays.
Is it too late for these countries and others? No. By applying the Hammer, they’re getting a new chance, a new shot at doing this right. The more they wait, the heavier and longer the hammer, but it can control the epidemics.
But what if all these measures aren’t enough?
The Dance of R
I call the months-long period between the Hammer and a vaccine or effective treatment the Dance because it won’t be a period during which measures are always the same harsh ones. Some regions will see outbreaks again, others won’t for long periods of time. Depending on how cases evolve, we will need to tighten up social distancing measures or we will be able to release them. That is the dance of R: a dance of measures between getting our lives back on track and spreading the disease, one of economy vs. healthcare.
How does this dance work?
It all turns around the R. If you remember, it’s the transmission rate. Early on in a standard, unprepared country, it’s somewhere between 2 and 3: During the few weeks that somebody is infected, they infect between 2 and 3 other people on average.
If R is above 1, infections grow exponentially into an epidemic. If it’s below 1, they die down.
During the Hammer, the goal is to get R as close to zero, as fast as possible, to quench the epidemic. In Wuhan, it is calculated that R was initially 3.9, and after the lockdown and centralized quarantine, it went down to 0.32.
But once you move into the Dance, you don’t need to do that anymore. You just need your R to stay below 1: a lot of the social distancing measures have true, hard costs on people. They might lose their job, their business, their healthy habits…
You can remain below R=1 with a few simple measures.

This is an approximation of how different types of patients respond to the virus, as well as their contagiousness. Nobody knows the true shape of this curve, but we’ve gathered data from different papers to approximate how it looks like.
Every day after they contract the virus, people have some contagion potential. Together, all these days of contagion add up to 2.5 contagions on average.
It is believed that there are some contagions already happening during the “no symptoms” phase. After that, as symptoms grow, usually people go to the doctor, get diagnosed, and their contagiousness diminishes.
For example, early on you have the virus but no symptoms, so you behave as normal. When you speak with people, you spread the virus. When you touch your nose and then open door knob, the next people to open the door and touch their nose get infected.
The more the virus is growing inside you, the more infectious you are. Then, once you start having symptoms, you might slowly stop going to work, stay in bed, wear a mask, or start going to the doctor. The bigger the symptoms, the more you distance yourself socially, reducing the spread of the virus.
Once you’re hospitalized, even if you are very contagious you don’t tend to spread the virus as much since you’re isolated.
This is where you can see the massive impact of policies like those of Singapore or South Korea:
- If people are massively tested, they can be identified even before they have symptoms. Quarantined, they can’t spread anything.
- If people are trained to identify their symptoms earlier, they reduce the number of days in blue, and hence their overall contagiousness
- If people are isolated as soon as they have symptoms, the contagions from the orange phase disappear.
- If people are educated about personal distance, mask-wearing, washing hands or disinfecting spaces, they spread less virus throughout the entire period.
Only when all these fail do we need heavier social distancing measures.
The ROI of Social Distancing
If with all these measures we’re still way above R=1, we need to reduce the average number of people that each person meets.
There are some very cheap ways to do that, like banning events with more than a certain number of people (eg, 50, 500), or asking people to work from home when they can.
Other are much, much more expensive economically, socially and ethically, such as closing schools and universities, asking everybody to stay home, or closing businesses.
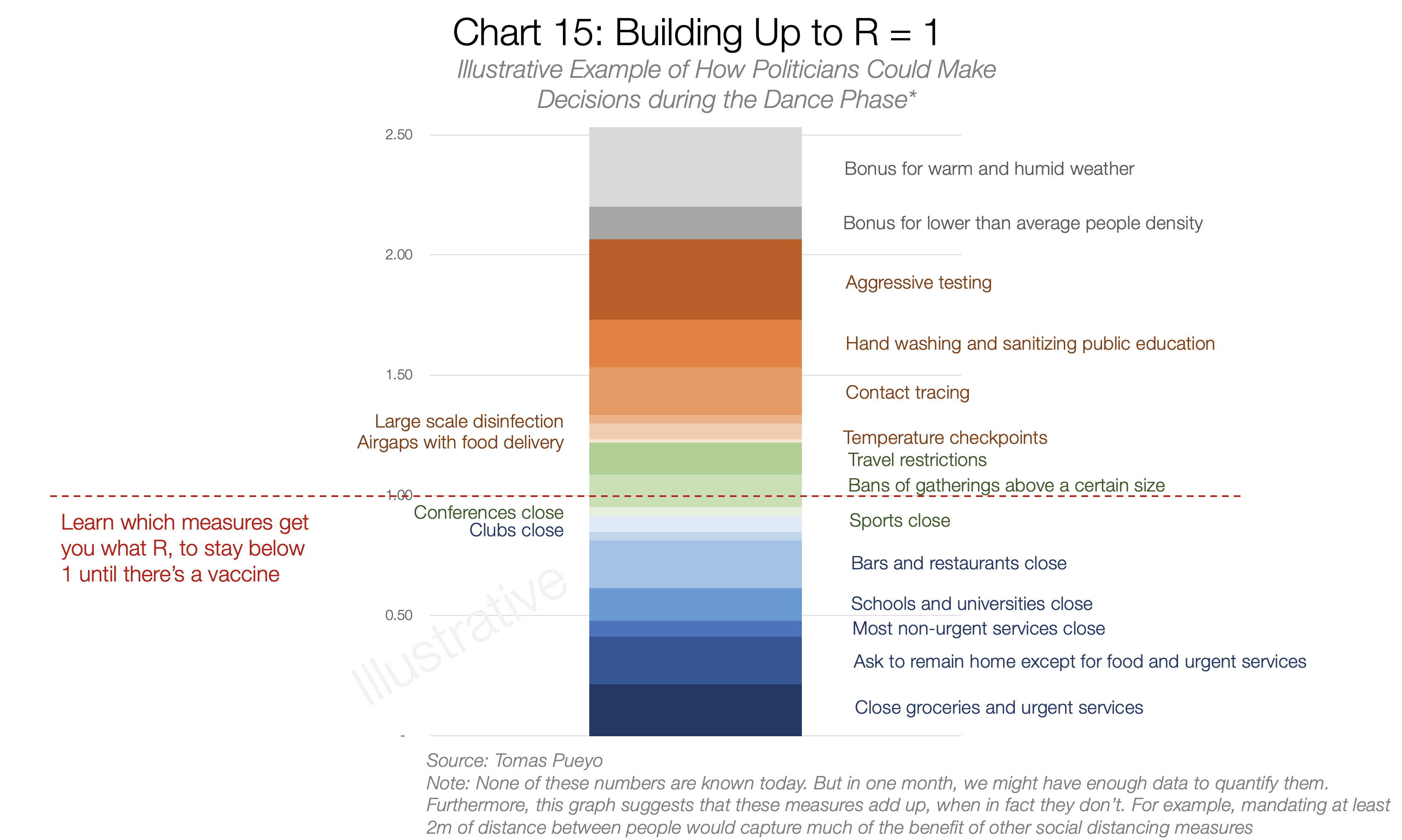
This chart is made up because it doesn’t exist today. Nobody has done enough research about this or put together all these measures in a way that can compare them.
It’s unfortunate, because it’s the single most important chart that politicians would need to make decisions. It illustrates what is really going through their minds.
During the Hammer period, politicians want to lower R as much as possible, through measures that remain tolerable for the population. In Hubei, they went all the way to 0.32. We might not need that: maybe just to 0.5 or 0.6.
But during the Dance of the R period, they want to hover as close to 1 as possible, while staying below it over the long term term. That prevents a new outbreak, while eliminating the most drastic measures.
What this means is that, whether leaders realize it or not, what they’re doing is:
- List all the measures they can take to reduce R
- Get a sense of the benefit of applying them: the reduction in R
- Get a sense of their cost: the economic, social, and ethical cost.
- Stack-rank the initiatives based on their cost-benefit
- Pick the ones that give the biggest R reduction up till 1, for the lowest cost.

This is for illustrative purposes only. All data is made up. However, as far as we were able to tell, this data doesn’t exist today. It needs to. For example, the list from the CDC is a great start, but it misses things like education measures, triggers, quantifications of costs and benefits, measure details, economic / social countermeasures…
Initially, their confidence on these numbers will be low. But that‘s still how they are thinking—and should be thinking about it.
What they need to do is formalize the process: Understand that this is a numbers game in which we need to learn as fast as possible where we are on R, the impact of every measure on reducing R, and their social and economic costs.
Only then will they be able to make a rational decision on what measures they should take.
Conclusion: Buy Us Time
The coronavirus is still spreading nearly everywhere. 152 countries have cases. We are against the clock. But we don’t need to be: there’s a clear way we can be thinking about this.
Some countries, especially those that haven’t been hit heavily yet by the coronavirus, might be wondering: Is this going to happen to me? The answer is: It probably already has. You just haven’t noticed. When it really hits, your healthcare system will be in even worse shape than in wealthy countries where the healthcare systems are strong. Better safe than sorry, you should consider taking action now.
For the countries where the coronavirus is already here, the options are clear.
On one side, countries can go the mitigation route: create a massive epidemic, overwhelm the healthcare system, drive the death of millions of people, and release new mutations of this virus in the wild.
On the other, countries can fight. They can lock down for a few weeks to buy us time, create an educated action plan, and control this virus until we have a vaccine.
Governments around the world today, including some such as the US, the UK or Switzerland have so far chosen the mitigation path.
That means they’re giving up without a fight. They see other countries having successfully fought this, but they say: “We can’t do that!”
What if Churchill had said the same thing? “Nazis are already everywhere in Europe. We can’t fight them. Let’s just give up.” This is what many governments around the world are doing today. They’re not giving you a chance to fight this. You have to demand it.
Share the Word
Unfortunately, millions of lives are still at stake. Share this article—or any similar one—if you think it can change people’s opinion. Leaders need to understand this to avert a catastrophe. The moment to act is now.
If you agree with this article and want the US Government to take action, please sign the White House petition to implement a Hammer-and-Dance Suppression strategy.
Buy Us Time to Fight the Coronavirus and Save Millions of Lives with a Hammer-and-Dance Suppression…
If you are an expert in the field and want to criticize or endorse the article or some of its parts, feel free to leave a private note here or contextually and I will respond or address.
If you want to translate this article, do it on a Medium post and leave me a private note here with your link. Here are the translations currently available:
Spanish (verified by author, full translation inc. charts)(alt. vs. 1, 2, 3, 4, 5, 6)French (translated by an epidemiologist)
Chinese Traditional (full translation including charts, alternative translation)Chinese Simplified
German
Portuguese (alternative version)Russian
Italian (with graphs translated)(Alternative 1, Alternative version on Facebook)
Japanese
Vietnamese
Turkish
Polish
Icelandic (alternative translation)Greek
Bahasa Indonesia
Bahasa Malaysia
Farsi (alternative version outside of Medium)
Czech (alternative translation)Dutch
Norwegian
Hebrew
Ukrainian (alternative version)Swedish
Romanian (alternative version)Bulgarian
Catalonian
Slovak
Filipino
Hungarian (Alternative, with part 1, part 2)
Chinese Traditional (full translation including charts, alternative translation)Chinese Simplified
German
Portuguese (alternative version)Russian
Italian (with graphs translated)(Alternative 1, Alternative version on Facebook)
Japanese
Vietnamese
Turkish
Polish
Icelandic (alternative translation)Greek
Bahasa Indonesia
Bahasa Malaysia
Farsi (alternative version outside of Medium)
Czech (alternative translation)Dutch
Norwegian
Hebrew
Ukrainian (alternative version)Swedish
Romanian (alternative version)Bulgarian
Catalonian
Slovak
Filipino
Hungarian (Alternative, with part 1, part 2)
This article has been the result of a herculean effort by a group of normal citizens working around the clock to find all the relevant research available to structure it into one piece, in case it can help others process all the information that is out there about the coronavirus.
Special thanks to Dr. Carl Juneau (epidemiologist and translator of the French version), Dr. Brandon Fainstad, Pierre Djian, Jorge Peñalva, John Hsu, Genevieve Gee, Elena Baillie, Chris Martinez, Yasemin Denari, Christine Gibson, Matt Bell, Dan Walsh, Jessica Thompson, Karim Ravji, Annie Hazlehurst, and Aishwarya Khanduja. This has been a team effort.
Thank you also to Berin Szoka, Shishir Mehrotra, QVentus, Illumina, Josephine Gavignet, Mike Kidd, and Nils Barth for your advice. Thank you to my company, Course Hero, for giving me the time and freedom to focus on this.
Stay on top of the pandemic
- Research: How Coronavirus is accelerating medical advances.
- Social distancing: Despite what the president says, staying home saves lives.
- Supplies: The paramedic in desperate need of face masks.
- Language: New coronavirus terms you might hear in the days to come.
Stay current with comprehensive, up-to-the-minute information, all in one place, at the new Medium Coronavirus Blog. Sign up for our Coronavirus newsletter here.
Thanks to Tito Hubert, Genevieve Gee, Pierre Djian, Jorge Peñalva, and Matt Bell.

WRITTEN BY
Follow
2 MSc in Engineering. Stanford MBA. Ex-Consultant. Creator of viral applications with >20M users. Currently leading a billion-dollar business @ Course Hero

/https://www.niagarafallsreview.ca/content/dam/thestar/news/canada/2021/09/25/huawei-executive-meng-wanzhou-receives-warm-welcome-upon-return-to-china/_1_meng_wanzhou_2.jpg)















No comments:
Post a Comment